The innovation process in hospital services: a case study in an occupational therapy
José Carlos Jacintho
jcj5847@gmail.com
Instituto Federal de Educação Ciência e Tecnologia – IFSP, São Paulo, São Paulo, Brazil.
Márcia Terra da Silva
e-mail: Márcia.terra@uol.com.br
Paulista University, São Paulo, São Paulo, Brazil.
Maria Cândida de Miranda Luzo
maria.candida@gmail.com
Orthopedics and Traumatology Institute, São Paulo, São Paulo, Brazil.
ABSTRACT
The theoretical debates in the literature point to the need of innovations in hospital services. The objective of this article is to identify the conditions of services that facilitate or hinder the process for different types of innovation in hospital services. For this, case studies were developed that allow the identification of the types of innovation found in the physical rehabilitation outpatient clinics of the Occupational Therapy unit (OT) of the Orthopedics and Traumatology Institute (OTI) of the Clínicas’ Hospital of the Faculty of Medicine of the University of São Paulo (HCFMUSP). The data collected reveal that the results of hospital services are related to the process of developing innovations in the various stages of the workflow, from the generation of ideas to the diffusion within the hospital unit. On the other hand, the review of the literature based on the reverse cycle of Barras and the complements of Gallouj and Djellal show that the paths of innovation in hospital services and innovations in industrial organizations are opposite. Therefore, the results of the analysis of the five cases selected for study reveal that, under the integrative approach, a process change leads to a product change. Thus, the article concludes that, in hospital services, innovations are born within the organizational structure as well as in external contact with professionals, researchers and surgeons.
Keywords: Innovation in hospital services; Types of innovation; Rehabilitation, Re-verse cycle, Hospital services.
INTRODUCTION
Gallouj (1998) questioned the ability of firms to effectively innovate in services, arguing that changes in service organizations could be understood only as modified results and values of the manufacturing activities. In view of this, Gallouj and Windrum (2009) and Gallouj and Savona (2009), question the specific need to create a new theoretical approach to service innovation.
On the other hand, if the service sector has a major importance in the world economic scenario, another question arises: do manufacturing theories support the process of innovation in services or an integrated approach that supports goods and services would be more suitable? To answer this question, it is important to know the paths of innovation in services and the conditions of use of technical, operational and organizational resources that support or hinder the innovation process.
It is in this context that innovations in hospital services are relevant, because, as Salge and Vera (2009) have shown, such organizations devote a great deal of attention to innovations, although they lack knowledge about its development. This lack is verified when analyzing the literature dedicated to hospital innovations, in which it is observed that the understanding of the innovation theme, in its majority, is directed towards medical innovations.
However, according to Djellal and Gallouj (2007), hospitals are complex service providers and health system hubs. Thus, according to the same authors, clients should be considered as consumers of a complex set of services to meet their particular and familiar needs. Thus, the understanding about innovations in services in hospital environments requires a holistic analysis of the hospital organization in all its aspects, that is, it should not only be limited to those directly related to medical activities, understood as techniques, but have other, related to support and organizational operations, such as rehabilitation, reception, hospitality, nutrition and communication.
This article investigates, through the study of cases of innovation, in the Occupational Therapy unit (OT) of the Institute of Orthopedics and Traumatology (OTI) of the Clínics’s Hospital of the Medical School of the University of São Paulo (HCFMUSP). The ideas for innovations in hospital services are generated, converted into effective results and disseminated by its stakeholders. The objective of the research is to identify service conditions that facilitate or hinder the process for different types of innovation.
THEORETICAL BACKGROUND
Many authors have used examples of service innovation, showing a multiplicity of types of innovation requiring different theoretical approaches to understand their processes.
For Gallouj (1998), three are the most indicated approaches: technicist, service-oriented (differentiation), and integrative. The first approach, the technicist, works on innovations in services such as manufacturing (tangible) technological conceptions and, according to Djellal et al. (2003), the incorporation of ICTs triggers non-technological innovations in organizations, requiring modifications in the organizational structure.
The main contribution to the understanding of this approach was elaborated by Barras (1986), with the "reverse product cycle" model, showing that the innovation in services runs in the opposite direction to that of technological innovation. Thus, Barras (1986) considers, in the first moment of the introduction of a new technology, the incremental process innovation aimed at improving efficiency, then radical innovation in processes, focusing on service quality, and, finally, the radical product innovation, resulting from new services or existing service recombination.
The second approach of Gallouj (1998) is service-oriented, and considers user-producer relations as the distinguishing feature of services production from manufacturing; so much so that, for Gallouj and Savona (2009), the first orientations for a Service-oriented innovation are the Knowledge Intensive Business Service (KIBS) and the ad hoc innovations.
The third approach of Gallouj (1998) is known as integrative and proposes the combination of goods and services to form a single theory of innovation. Therefore, the theory about the management of services puts the presence of the client and the intangibility of the results as operating conditions. The tendencies point to the concept that "product" is the end result, that is, the solution to the problem of the patient or client, be it a good (tangible) or a service (intangible), according to BRAX (2005), SPRING and ARAÚJO (2009), TUKKER (2004) and PAWAR, BELTAGUI and RIEDEL (2009).
According to Gallouj and Savona (2009), the integrative approach is one that offers the best conditions for the theoretical development of innovation in services; however, the authors emphasize that, if the specific needs of the customer are met by the consumption of goods, services or both, the distinction between both is unnecessary.
However, Gallouj and Weinstein (1997) show that the provision of a given service can be understood as the result of a final technical characteristics obtained from the combination of the technical characteristics that mobilize certain competencies. The authors emphasize that the participation of the client in co-production is one of the main characteristics of the provision of services when shared to the production of certain goods.
Figure 1. Representation of a product
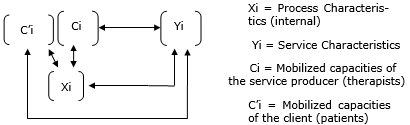
Source: Gallouj and Weinstein (1997)
However, for Zuckerman et al. (2013), a particular importance shall be the recognition of user-led innovation, a concept that shows the innovation process made by a small but significant percentage of users. In this case, user-led innovation is very important because the health care professionals and patients have an intimate perception of problems, needs and of the possible solutions.
In figure 1, Xi represents a set of technical characteristics with the following meanings: tangible technical characteristics of front-office; tangible technical back-office features and the intangible technical characteristics of front-office and back office, as well as organizational characteristics. Yi represents the set of final characteristics, obtained by a combination of technical characteristics Xi. Ck are the mobilized competencies of the service provider, while the term C'k represents the competencies of the customer.
On the other hand, Hansen and Birkinshaw (2007) emphasize that the integrative approach suggests that value creation for service organizations may be embedded in an innovation value chain, consisting of generating ideas, converting them into products and disseminating practices and products obtained by the organization.
Table 1. Innovation value chain

Source: Adapted for Hansen and Birkinshaw (1997)
It is important to note that, for Sundbo and Gallouj (1998), there may be product, process, organizational or market innovation, and according to Gallouj and Weinstein (1997), if the product is a set of characteristics, innovation will be any change that has the potential to impact such characteristics. The intensities considered can be radical, improvement, incremental, ad hoc, recombination or formalization.
On the other hand, Djellal and Gallouj (2005, 2007) propose a more dynamic understanding of innovation in hospital environments. They expand their definition to other forms, not only the techniques and technologies of medical practices, but also organizational with varying degrees of intensity, such as radical, incremental or improvement. Thus, the outputs of the hospital services, for Djellal and Gallouj (2005), must meet the following variables:
a) Component of the services provided within the hospital organization (Si): the most important are the medical, hotel, and nutrition services, administrative and managerial services;
b) Means of service delivery, corresponding operations or functions and associated technologies:
b.1) Material (M): material operations with corresponding sciences and technologies, logistical and material transformation that involve the processing of tangible objects, that is, transporting, transforming, maintaining or repairing them;
b.2) Informational (I): informational operations with corresponding sciences and technologies, logistical and information processing that involve the gathering and processing of codified information, that is, producing, capturing, transporting, archiving, and updating it;
b.3) Methodological (K): methodological operations with corresponding sciences and technologies, involving the intellectual processing of knowledge, using codified methods and routines and intangible technologies;
b.4) Relational (R): contacting or relational service operation with corresponding sciences and technologies and service operations in which the principal medium is the customer and which consists of a direct service provided in contact with the customer and with a greater or lesser degree of interaction;
c) Competences mobilized of service producers (C) or clients (Ci): are the professional skills, individual or team that operates in the hospital organization and often are expressed tacitly, so difficult to identify. These competences are derived from various sources: initial education and training, continuing training, experience and, more generally, the various interactions that are sources of learning.
d) Final characteristics of the service (Y): this is the value generated to the customer and perceived by him; indicates the usefulness of a particular service component. It is the result of combining the means of providing services (M, I, K, R) and competences mobilized skills (C; Ci). In service activities the task of identifying and labelling them may vary in terms of difficulty, depending on the type of constituent service in question. If the hospital service, as a whole, is adopted as the unit of analysis, then it can be defined as a package type of service. In this case, a simple way of denoting the service characteristics is to represent them in terms of the various constituent services or functions that make up the package.
e) Interorganizational and intraorganizational relationships: these are the relational aspects that involve the interactions between the stakeholders in different environments, both internal and external to hospitals, as Chesbrough (2003) points out in open innovation.
On the other hand, Lambooij and Hummel (2013) show that a service, including hospital service, can be understood as the result of a combination of technical characteristics obtained from the combination of operations and competencies of the service providers and the patient or client in its co-production.
However, according to Lambooij and Hummel (2013), many innovations applied to hospital services do not affect target groups; they are not applied in daily practice and do not provide benefits to the actors involved, because there is no policy and balance of power among stakeholders that consider a social deployment and not only technique of innovation, which creates negative impacts on the speed and diffusion of innovations in the organization.
METHODOLOGY
In order to reach the objectives of the article, the research focused on the innovation process of the rehabilitation clinics of the Occupational Therapy units of the Orthopedics and Traumatology Institute (OTI) of the Clinics’s Hospital of the University of São Paulo (HCUSP).
Because it is a Public University Hospital, HCUSP offers favorable conditions for the development of academic work and, by working with several specialties, enables the researcher to contact a variety of situations to enrich the research.
The proximity to IOT researchers allowed the identification of better working conditions and a space not yet explored for the discussion of innovation processes in hospital services.
On the other hand, the dynamics of the activities of the Occupational Therapy unit of the Orthopedics and Traumatology Institute, its proximity to the development of medical research and the interest of its professionals in the innovation processes coincided with the interests of this research.
The first step was the recognition of the field of research, that is, an attempt was made to understand the meaning, functions, differences, and importance of Occupational Therapy as support activities of orthopedic trauma or post-surgical treatments and in the rehabilitation of patients. Field research, at this stage, focused on the rehabilitation in outpatient clinics of the Occupational Therapy units of the Orthopedics and Traumatology Institute.
During the months of September, October and November of 2016 and January 2017, about 10 hours per week were devoted to field research. From there, the research developed in two parts: a theoretical conceptual basis on innovation in hospital services and qualitative data collection in the respective outpatient clinics.
Field surveys were developed in three moments: the first was observational, the second was devoted to interviews with directors and coordinators of the unit, and the third was interviews with the therapists.
Among the innovations identified in the studied environment, five were analyzed under the integrative approach of Gallouj (1994) and Gallouj (1998). These cases are representative of the innovation value chain in different aspects, such as: where and how the generation of the idea occurred; if there was the participation of external professionals or patients, and how the idea was disseminated in the Occupational Therapy unit.
The final analysis of the information and data collected were shared and validated with the director responsible for the Occupational Therapy unit. In this way, each identified innovation process created potential for sharing and diffusion throughout the unit.
The bibliographical references found for the topic under study refer to classic articles that show the state of the art for innovation in hospital services. As the theoretical basis on innovation in hospital services is not fully consolidated, this article hopes to contribute through the analysis of the practical cases studied.
RESULTS AND DISCUSSIONS
Among the innovations identified in the studied environment, five innovations were selected, according to table 2. The analysis of these innovations will be discussed in light of the "reverse product cycle", a model proposed by Barras (1986), the framework developed by Djellal and Gallouj (2007), and the first theories of Gallouj (1998) for innovation in services.
Table 2. Innovation cases identified in the Occupational Therapy Unit

Source: prepared by the authors
- Orthoses laboratory
The material that requires higher processing temperatures in favor of greater flexibility, combination of materials, higher quality, longer durability, higher stiffness, and shorter processing time.
The laboratory is a good example of the application of technological innovation in services, reinforced by the evidences of the three phases of the reverse product cycle of Barras (1986): first, the efficiency improvement, obtained by training the team of therapists to characteristics of the new process; the mastery of the new process leads to the maturity of knowledge regarding 3D printing, that is, since it is a new and totally different process from the existing process. Finally, in a third phase, it will be possible to create a new material orthosis, which will result in a new way of providing orthotic services to patients, reduction in the time of manufacture and increase in the quality of the product, providing greater patient comfort, durability and flexibility of use.
- Process of care
Objective: to adjust to the availability of specialized personnel to autonomy and functionality.
This innovation reveals the relational and patient character of the therapist, the co-production of the service, the particularity of being ad hoc, as well as highlighting the specialized knowledge-intensive service (KIBS) of occupational therapists. These are packages of services rendered directly to the patients, but demanded by the physicians of the outpatient clinic.
- Ankle and Foot orthosis of Weil
Objective: Leverage medical outcomes and outpatient rehabilitation for ankle and foot surgery. This innovation has an essentially technical surgical character. These are new therapeutic procedures for foot rehabilitation that require the use of orthoses to maximize treatment results, allowing greater functionality and autonomy for patients. In this process, the expertise and competences of the therapists contributed decisively to the success of the surgical result. Therefore, as it was a new experience, generated from the partnership between the Occupational Therapy unit and the orthopedic surgeons, it can be considered as a radical, integrative, interorganizational innovation, the result of which is a new product of the hospital service offered to patients. It is a type of knowledge-intensive service (KIBS).
- Clinical Research - post-surgical treatment for correction of Dupuytren's disease.
Objective: To compare the treatment and behavior of patients who underwent classical surgery and stem cell surgery. Because it is a research order, it can be considered that this innovation is radical, with an integrative approach of Gallouj (1994) and interorganizational. On the other hand, the reverse cycle of the product of Barras (1986) is verified, as it seeks to improve efficiency in post-surgical rehabilitation, followed by a new knowledge and reach of maturity, characterizing a radical innovation and finally the generation of a new product of the service applied, represented by the new protocols for the surgical process and for the post-surgical rehabilitation.
- Annual Operations Planning:
Objective: To improve the critical processes of the Occupational Therapy unit.
It is an incremental and intraorganizational innovation, to improve the critical processes of the Occupational Therapy unit. The actions developed aim at the delivery of a new form for appointment scheduling or high patient clinics. On the other hand, therapists seek to be able to improve the performance of the billing system through courses that generate revenues by disseminating knowledge to external clients.
Table 3 shows a framework of the functional and relational division of innovation for each of the innovations described in Table 2, with reference to the work of Djellal and Gallouj (2007).
Table 3. Framework functional and relational division of OT outputs

Source: adapted from Djellal and Gallouj (2005)
Thus, from framework shown in the table 3 for this research:
Si is the services provided by the OT unit:
-
New process for orthoses conceived from the laboratory;
-
Process of care for rehabilitation and processes to receive the patient (reception);
-
Ankle and foot orthosis (Weil) a surgery technique and a new field of knowledge within the surgical procedures;
-
Clinical research a post surgical treatment for Dupuytren’s disease; for the occupational therapy unit there will be new rehabilitation techniques;
-
Annual operations planning is a special meeting of OT work team for planning new routines and innovations.
Yi are the expected results with innovation and they generate value for patients - Yi = f (Ci, Mi, Ii, Ki, Ri):
-
To produce orthoses with different types of materials;
-
To adjust to the availability of specialized personnel and allow greater autonomy and functionality to the patients;
-
Leverage medical outcomes and outpatient rehabilitation for ankle and foot surgery;
-
To compare the treatment and behavior of patients who underwent classical surgery and stem cell surgery;
-
To improve the critical processes of the Occupational Therapy unit.
Ci is the new knowledge acquired with innovation or mobilized capacities of the service producer (therapists and patients):
Service means are operations: (Ii) methodological operations; (Ki) creation of new routines; (Ri) Relational operations; and (Mi) Materials and equipment used.
Organizational level (Oi) external/internal partnerships: therapist relationships among themselves or with patients and surgeons.
CONCLUSIONS
This article identified and analyzed five innovations in the Occupational Therapy unit of the IOT during the period studied. The studies pointed out that the processes of innovation dealt with the integrative approach, according to Gallouj (1998) and Gallouj (1994), as well as the assumptions of the "Reverse cycle of the product" of BARRAS (1986). On the other hand, the development of research shows that innovations are achieved according to the innovation value chain studies of Hansen and Birkinshaw (1997).
In the product and processes innovations evaluated, the relative effectiveness was observed and the patient, through co-production, contributed to the success of his own treatment. The interaction between therapists, patients, and surgeons was one of the success factors of the innovations analyzed.
The innovations were born from ideas to improve processes, generated within the OT team and from external demands, such as those of orthopedic surgeons. For the OT team the innovations represented opportunities for professional growth and effectiveness in the treatments of each patient. For surgeons, however, innovations were opportunities for improving outcomes in post-surgical complications.
The main difficulty encountered during the research was to establish a criterion for identifying innovations, since the idea that innovation should be technological and that it would only make sense if innovation was radical prevailed.
REFERENCES
Barras, R. (1986), “Towards a theory of innovation in services.”, Research Policy, Vol.15, pp. 161-73.
Brax, S. (2005), “A manufacturer becoming service provider – challenges and a para-dox.”, Managing Service Quality, Vol.15, No.2, pp. 142-55.
Djellal et al. (2003), “Revising the definition of research and development in the light of the specifities of services.”, Science and Public Policy, Vol.30, No.6, pp. 415 – 30.
Djellal, F.; Gallouj, F. (2005), “Mapping innovation dynamics in hospitals.”, Research Poli-cy, No.34, pp. 817–35.
Djellal, F.; Gallouj, F. (2007), “Innovation in hospital: a survey of the literature.”, Europe-an Journal of Health Economics, No.8, pp. 181 – 93.
Gallouj, F. (1994), Innovation dans les services, L’Harmattan, Paris.
Gallouj, F. (1998), “Innovating in reverse: services and the reverse product cycle.”, Euro-pean Journal of Innovation Management, Vol.1, No.3, pp.123.
Gallouj, F.; Savona, M. (2009), “Innovation in service: a review of the debate and a re-search agenda.”, Journal of Evolutionary Economics, Vol.19, No.2, pp. 149 – 72.
Gallouj, F.; Weinstein, O. (1997), “Innovation in services”, Research Policy, Vol.2, pp. 537 – 56.
Gallouj, F.; Windrum, P. (2009), “Services and Services Innovation.”, Journal of Evolu-tionary Economics, Vol. 19, pp. 141–8.
Hansen, M. T.; Birkinshaw, J. (2007), “The innovation value chain”, Harvard Business Re-view, Vol.85, No.6, pp.121-30.
Lambooij, M. S.; Hummel, M. J. (2013), “Differentiating innovation priorities among stake-holder in hospital care”, BMC Medical Informatics and Decision Making, Vol. 13, pp. 91.
Pawar, K. S. et al. (2009), “The PSO triangle: designing product, service and organization to create value”, International Journal of Operations & Production Management, Vol. 29, No. 5, pp. 468 – 93.
Salge, T.O.; Vera, A. (2009), “Hospital Innovativeness and organizational performance: evidence from English public acute care”, Health Care Management Review, Vol. 34, No. 1, pp. 54 – 67.
Spring, M; Araújo, L. (2009), “Service, services and products: rethinking operations strat-egy.”, International Journal of Operations & Production Management, Vol. 29, No. 5, pp. 444 – 67.
Sundbo, J; Gallouj, F. (1998), Innovation in service, PREST – Policy Research in Engineer-ing, Scence & Technology, Manchester.
Tukker, A. (2004), “Eight types of product-service system: eight ways to sustainability experiences from suspronet”, Business Strategy and the Environment, No.13, pp. 246-60.
Zuckerman, B. et al. (2013), “Health services innovation: the time is now”, JAMA, Vol. 309, No. 11.
Received: 02 Apr 2018
Approved: 08 May 2018
DOI: 10.14488/BJOPM.2018.v15.n2.a14
How to cite: Jacintho, J. C. (2018), “The innovation process in hospital services: a case study in an occupational therapy”, Brazilian Journal of Operations & Production Management, Vol. 15, No. 2, pp. 322-329, available from: https://bjopm.emnuvens.com.br/bjopm/article/view/475 (access year month day).